
Equine athletes spend many hours either preparing for a competition or event, or competing in the event. Like human athletes this level of preparation stresses all the body systems, in particular the musculoskeletal system. With horses, lameness originating from either joint soreness, or tenderness involving certain tendons and ligaments, is common. But as in humans, soreness arising from skeletal muscles is also common. Some muscle soreness seems to be activity specific (sore pectoral muscles in jumping horses), but often the large muscle groups of the back and gluteal region, and occasionally the hamstring muscles, are affected. Muscle soreness can be primary in origin, or secondary to lameness issues that can alter the way the horse moves, leading to secondary muscle soreness.
Veterinarians are best suited to diagnose and treat the lameness issues, and many who work on equine athletes also have experience with muscle soreness issues. Many veterinarians have taken further training in acupuncture and/or what is often referred to as manual therapy (chiropractic work, osteopathy or physical therapy), which allows them to assess and treat muscle soreness in a different manner than their veterinary medical training provided. Non-veterinarians also participate in working on body soreness issues, and many of these individuals are experienced and competent. However little to no targeted training is required to attach the term ‘body worker’ to one’s name, so careful scrutiny should be employed before having just anyone work on your horse.
Primary Modalities – Chiropractic/Osteopathy
Both of these modalities address predominantly what is referred to as the axial skeleton versus the appendicular skeleton. The axial skeleton includes the neck, back and pelvis, whereas the appendicular skeleton refers to the limbs. Both entities may be concurrently involved, so again it is important to ensure that lameness originating in the limbs is not the major issue before spending considerable time and effort addressing only the axial skeleton.
In large part, both of these modalities evaluate the movement or motion characteristics of the axial skeleton. Both use some version of a ‘motion palpation’ to try and locate areas of restricted movement or motion affecting the neck, back and pelvis. Both also include a motion assessment of the limbs, but the axial skeleton is the major area being addressed. The motion palpation helps identify areas where normal movement feels restricted (and less often where hypermobility may be present), and treatment is then addressed using ‘adjustments’ to try to restore movement to the affected area.
Restricted movement arises when some of the soft tissues that surround a certain segment of the axial skeleton become tight and less flexible. This may result from a specific injury to those tissues, or it may arise secondarily to the tissue shortening that arises when an area is secondarily ‘guarding’ to help accommodate a soreness problem elsewhere. This reinforces why it is necessary to make sure a primary problem is not overlooked while all efforts address the secondary issue. Whether the ‘tissue shortening’ is primary or secondary, ultimately some type of manipulation may be necessary to help restore mobility to the affected region. The shortening refers to the contracted state that local muscles and ligaments may assume to help guard or restrict movement in that local area until either local healing is sufficient, or the other primary remote problem is addressed, to allow the area of tissue shorting to return to normal. Unfortunately such areas do not always return to normal, requiring some type of intervention to help restore normal mobility.
Techniques
In chiropractic, the adjustment technique is called a ‘high velocity, low amplitude’ (HVLA) adjustment. This is a sharp manual thrust directed at the area of restricted mobility that is designed to input a new and different signal to the ‘shortened ‘ tissues, to signal that this shortened, restricted state is no longer required. Osteopathy uses some HVLA technique but also relies more on what is referred to as ‘long-lever’ technique, where the limbs are taken through large ranges of motion to exert an effect at the axial skeleton level. These ‘long-lever’ adjustments are used to excess by some minimally trained body workers, who rely on heavy horse sedation and aggressive limb manipulation, to complete a ‘treatment’. Neither sedation or aggressive limb manipulation are required in these horses, so this type of approach should be avoided.
Target Areas
In both modalities, a major target tissue of therapy is what is referred to as the ‘postural’ muscles that invest the vertebrae of the neck and spine.
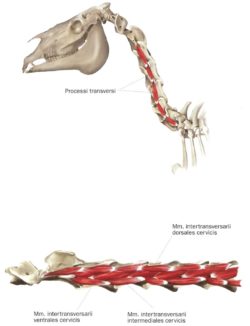
These muscles control the small but highly controlled micro-movements between the various vertebral segments, and are a large part of what becomes restricted in ‘tissue shortening’. Although it is generally the larger surface muscles (the mobilizer muscles) that are used to determine soreness it is often the deeper postural muscles that need to be addressed to restore mobility.
Treatments
Sometimes more than one treatment or adjustment is required for success, but often a single treatment can restore the desired mobility. Restricted exercise may be temporarily required in certain cases where soreness has been severe, but generally a return to use is desired so that the regained mobility can be retained. If there are attendant lameness issues, or tack fit or rider issues, those need to be concurrently addressed.
There are other modalities that can be used concurrently with or separate from chiropractic or osteopathic work. These include but are not restricted to massage and other soft tissue manual therapies, acupuncture and physical therapy. What is available in a certain area will help guide this decision as will input from your veterinarian or trusted colleagues. Remember, ask your veterinarian, and don’t forget to do a little carefully considered Googling!
Comments are closed